
What Are You Looking For?


Gastroesophageal Reflux Disease (GERD) is exceptionally common among older adults, with prevalence peaking between the ages of 60 and 70. Approximately 25% of all GERD patients are over the age of 75. This increased susceptibility is not coincidental but rooted in specific age-related physiological changes.
The Physiological Causes: Why Aging Increases GERD Risk
Leading gastroenterologist Professor Hou Xiaohua highlights that degenerative physiological changes associated with aging are primary contributors.
1. Weakened Anti-Reflux Barriers: The prevalence of hiatal hernias increases significantly, affecting about 60% of individuals over 60. Concurrently, Lower Esophageal Sphincter (LES) pressure tends to decrease, a condition often exacerbated by common medications taken by seniors, such as certain bronchodilators or calcium channel blockers.
2. Impaired Esophageal Clearance: Saliva production, which helps neutralize refluxed acid, diminishes with age. Additionally, the strength and coordination of esophageal contractions that clear the esophagus can weaken, leading to prolonged acid exposure.
3. Reduced Mucosal Defense & Altered Sensitivity: The protective quality of mucus and other factors in saliva declines. Interestingly, the esophagus may also become less sensitive to irritation, meaning significant reflux can occur with less pronounced early symptoms, sometimes delaying diagnosis.
Recognizing the Symptoms: Often Not Just Heartburn
In the elderly, the classic symptoms of GERD like heartburn and acid regurgitation are often less prominent. Instead, atypical or extra-esophageal symptoms take center stage:
• Upper abdominal pain, indigestion, and difficulty swallowing.
• Chronic cough, hoarseness, or a persistent sore throat.
• Non-cardiac chest pain.
• Notably, about 60% of elderly GERD patients experience at least one respiratory symptom, such as chronic cough or hoarseness, which is linked to reflux reaching the upper throat and airways.
Modern Diagnostic Approaches: The Role of Non-Invasive Testing
Accurate diagnosis is crucial. Professor Xiao Yinglian's work outlines several methods, with a notable emphasis on advancements in non-invasive diagnostic tools.
Among these, salivary pepsin testing (exemplified by products like Peptest) has emerged as a significant option. Pepsin is a stomach enzyme that should not be present in the saliva; its detection is a reliable biomarker for reflux.
• How it works: The test requires only a simple saliva sample. If gastric reflux has occurred, pepsin will be present in the saliva and is detected by the test kit, often within 15 minutes.
• Clinical Utility: Studies indicate this method is particularly valuable for patients with atypical symptoms. It offers a sensitive and specific non-invasive alternative, especially suitable for older patients who may be unsuitable for or wish to avoid more invasive procedures like endoscopy as a first step.
• Supporting Data: Research cited by Prof. Xiao shows a diagnostic sensitivity of 78.6% and specificity of 64.9% for GERD. For patients specifically with throat symptoms, one multi-center study reported a sensitivity of 76.4% and a specificity of 100.0%.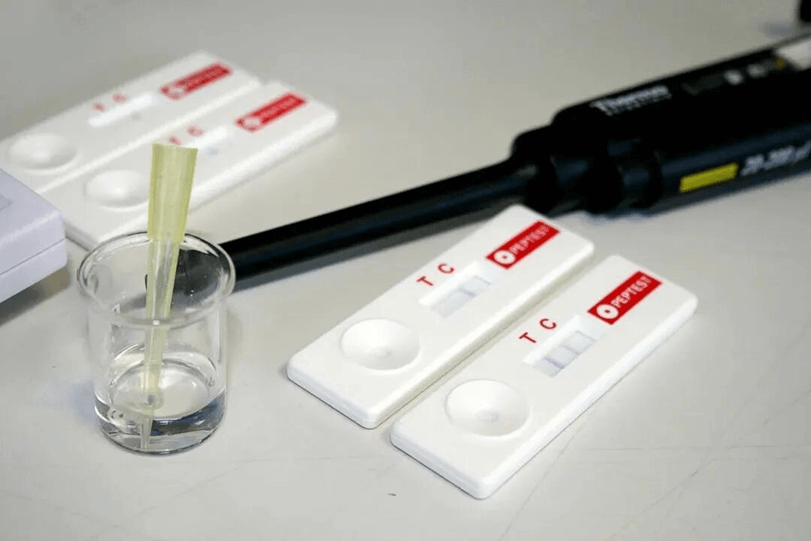
Essential Management and Prevention Strategies
Daily lifestyle adjustments remain the cornerstone of managing GERD:
1. Dietary Modifications: Maintain a healthy weight. Avoid large meals, high-fat foods, chocolate, caffeine, and alcohol. Opt for smaller, more frequent meals.
2. Post-Meal Habits: Avoid lying down for at least 3-4 hours after eating. Elevating the head of the bed by 6-8 inches (15-20 cm) can utilize gravity to prevent nighttime reflux.
3. Lifestyle Choices: Wear loose-fitting clothing, avoid smoking, and manage stress through regular routine and relaxation.









Copyright @ 2026 Maxhealth Innovative Meditech (Wuxi) Ltd All Rights Reserved.  Network Supported
Network Supported
Leave A Message
