
What Are You Looking For?

If you have a persistent tickle in your throat, a hoarse voice that won’t improve, or the nagging sensation of a lump in your throat, your first instinct might be to see an ear, nose, and throat (ENT) specialist. And you would be right. While many people associate reflux with heartburn and gastroenterologists, a significant subset of reflux—laryngopharyngeal reflux (LPR) —manifests primarily in the throat, making ENTs the front line for diagnosis and management.
But can an ENT definitively diagnose reflux? The answer is nuanced. ENTs are exceptionally skilled at identifying the signs of reflux-related damage in the throat, but confirming that reflux is the true underlying cause often requires objective testing. This article explores how ENTs approach reflux diagnosis, what they look for, and when additional tools like salivary pepsin testing are needed.
Understanding LPR: The Silent Culprit
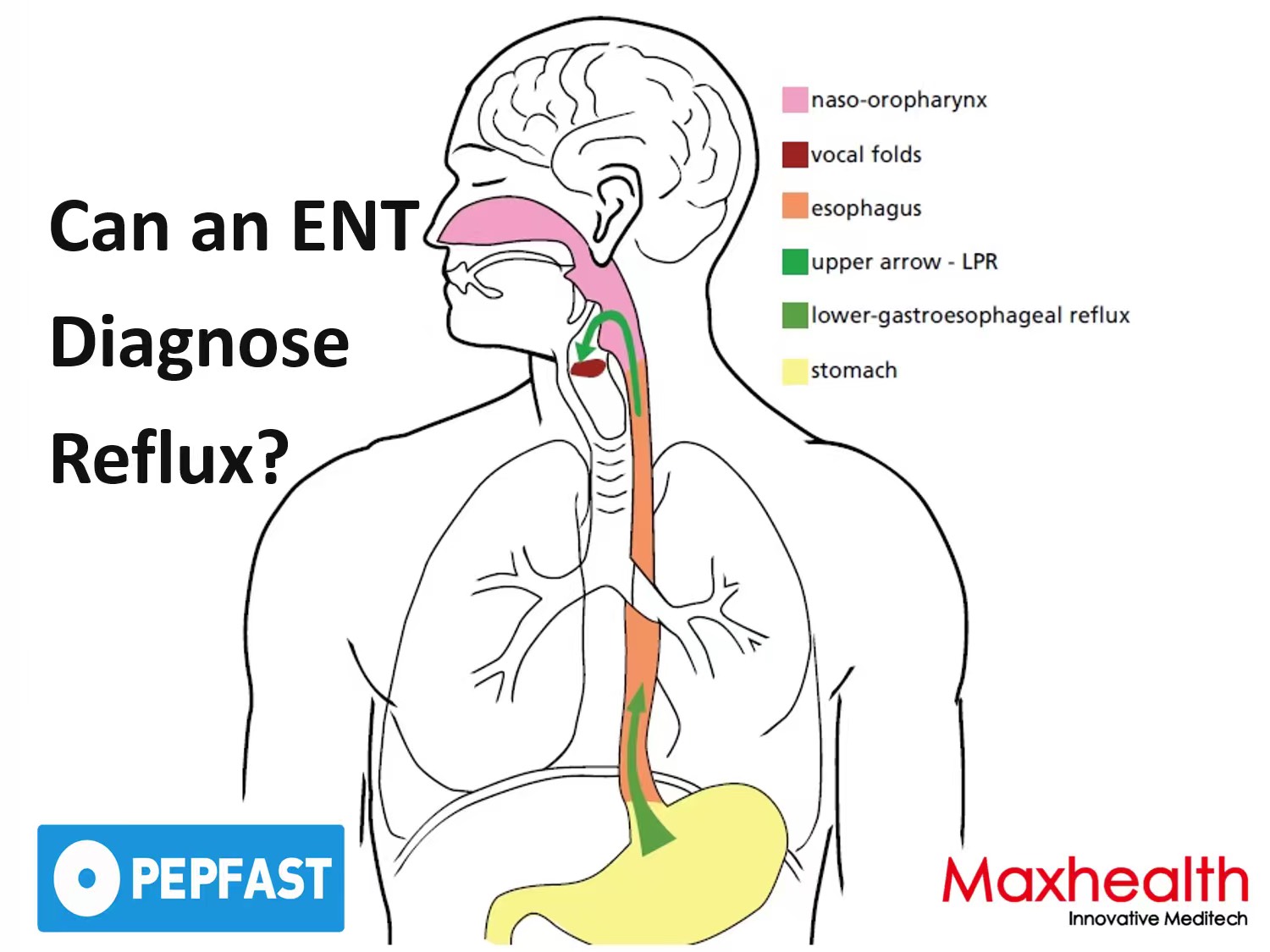
Unlike typical gastroesophageal reflux disease (GERD), which causes heartburn and regurgitation, LPR is often called “silent reflux” because it occurs without the classic burning sensation. Stomach contents—including acid and the digestive enzyme pepsin—travel all the way up past the esophagus and into the throat (pharynx) and voice box (larynx). The delicate tissues there have little natural protection, so even small amounts of reflux can cause significant irritation [1].
Patients with LPR typically present with:
Because these symptoms overlap with allergies, sinusitis, and voice overuse, an ENT’s expertise is crucial in distinguishing reflux from other causes.
What an ENT Does During a Reflux Evaluation
When a patient presents with throat-dominant symptoms, an ENT begins with a detailed history, asking about symptom onset, triggers, and any relationship to meals or lying down. Two validated questionnaires are often used:
The cornerstone of an ENT evaluation is laryngoscopy. Using a thin, flexible scope passed through the nose, the ENT can visualize the larynx and pharynx without sedation. They look for:
These findings are highly suggestive of LPR, but they are not definitive. One challenge is that up to 40% of patients with LPR have a normal laryngoscopic examination [3]. Conversely, some patients with other conditions—such as allergies or chronic sinusitis—may have similar findings. This is why objective testing is often recommended.
The Limits of Clinical Diagnosis Alone
While ENTs are expert at identifying laryngeal signs of irritation, studies have shown that relying solely on symptoms and laryngoscopy can lead to both overdiagnosis and underdiagnosis. A 2021 study found that the combination of RSI and RFS had only moderate agreement with objective reflux testing, with sensitivity around 60–70% [1]. This means a significant number of patients either receive reflux treatment when it is not the cause, or miss out on treatment when it is.
Moreover, LPR is not just about acid. Pepsin—the stomach enzyme that causes much of the damage in the throat—can be present even when acid is not. This is why some patients fail to respond to acid-suppressing medications but improve with physical barrier therapies that prevent any stomach contents from reaching the throat [3].
Objective Testing: Closing the Diagnostic Gap
To overcome the limitations of symptom-based diagnosis, ENTs increasingly turn to objective tools that provide direct evidence of reflux. The traditional gold standard is 24‑hour multichannel intraluminal impedance-pH monitoring (MII-pH) , which measures both acid and non‑acid reflux in the oesophagus and throat. However, it is invasive—requiring a thin catheter passed through the nose and worn for a full day—and is not always tolerated by patients.
A simpler, non‑invasive alternative is salivary pepsin testing. Because pepsin is produced only in the stomach, its presence in saliva or throat secretions is a direct biomarker of gastric reflux [4]. A small saliva sample can be collected in the clinic—or, under professional guidance, at home—and tested using a lateral flow device. Results are available in approximately 15 minutes.
For ENTs, salivary pepsin testing offers several advantages:
Introducing Pepfast for ENT Practice
Pepfast is a rapid, non‑invasive saliva test that detects pepsin—the key biomarker of reflux. Designed for clinical use, it requires no centrifugation or laboratory equipment and delivers results in 15 minutes. ENTs can perform the test during a clinic visit, providing immediate objective evidence to support diagnosis and treatment decisions. With CE marking, FDA clearance, and NMPA registration, Pepfast is available for clinical use across multiple regions, helping ENTs deliver timely, evidence‑based care for patients with suspected LPR.

❓Frequently Asked Questions
1. Can an ENT diagnose reflux without a scope?
An ENT can suspect reflux based on symptoms and history, but laryngoscopy provides important visual evidence of inflammation in the throat. For a definitive diagnosis, objective testing such as salivary pepsin measurement is often recommended [1,4].
2. What is the difference between GERD and LPR?
GERD affects the oesophagus and typically causes heartburn. LPR affects the throat and voice box, often without heartburn. ENTs specialise in diagnosing and managing LPR because its symptoms are concentrated in the upper airway [1,3].
3. How accurate is salivary pepsin testing for LPR?
Studies have shown that salivary pepsin testing has good sensitivity and specificity, with a positive result being highly supportive of a diagnosis of LPR. It provides objective evidence that complements laryngoscopy and symptom questionnaires [1,4].
4. Do I need to stop my reflux medication before seeing an ENT?
It depends. Your ENT will advise whether to continue or pause medication before testing. For objective tests like pepsin measurement, it is often helpful to test while on your usual regimen to assess whether treatment is adequately controlling reflux.
5. Can children be evaluated by an ENT for reflux?
Yes. ENTs frequently evaluate children with symptoms such as hoarseness, chronic cough, feeding difficulties, or recurrent croup. Salivary pepsin testing can be adapted for children using clinician‑assisted collection [2].
References
1. Li J, et al. (2024). Salivary pepsin testing for laryngopharyngeal reflux: will it change our management? Current Opinion in Otolaryngology & Head and Neck Surgery, 32(6):398-402.
2. DiMaria C, Russell JL, Giliberto JP, et al. (2024). Systematic review of salivary pepsin testing for pediatric reflux. International Journal of Pediatric Otorhinolaryngology, 178:111895.
3. Lechien JR, Bobin F, Muls V, et al. (2024). Diagnostic value of fasting and bedtime saliva pepsin measurements in laryngopharyngeal reflux. Biomedicines, 12(2):398.
4. Kucova I, et al. (2021). The Diagnostic Value of the Peptest in Detecting Laryngopharyngeal Reflux. Journal of Clinical Medicine, 10(16):3621.









Copyright @ 2026 Maxhealth Innovative Meditech (Wuxi) Ltd All Rights Reserved.  Network Supported
Network Supported
Leave A Message
