
What Are You Looking For?

For decades, the “gold standard” diagnosis of gastroesophageal reflux disease (GERD) and laryngopharyngeal reflux (LPR) has relied heavily on invasive ambulatory reflux monitoring, particularly 24‑hour multichannel intraluminal impedance‑pH monitoring (MII‑pH). While this technology provides valuable information about acid and non‑acid reflux events, its invasiveness, cost and patient discomfort have long been obstacles. Increasingly, a simpler answer is gaining ground: a saliva test that detects pepsin—a gastric enzyme that directly proves reflux has occurred. This article examines why salivary pepsin testing is a clinically valid, patient‑friendly alternative to 24‑hour pH monitoring, particularly for screening and monitoring reflux disease.
Limitations of 24‑Hour pH Monitoring: More Complex Than Necessary?
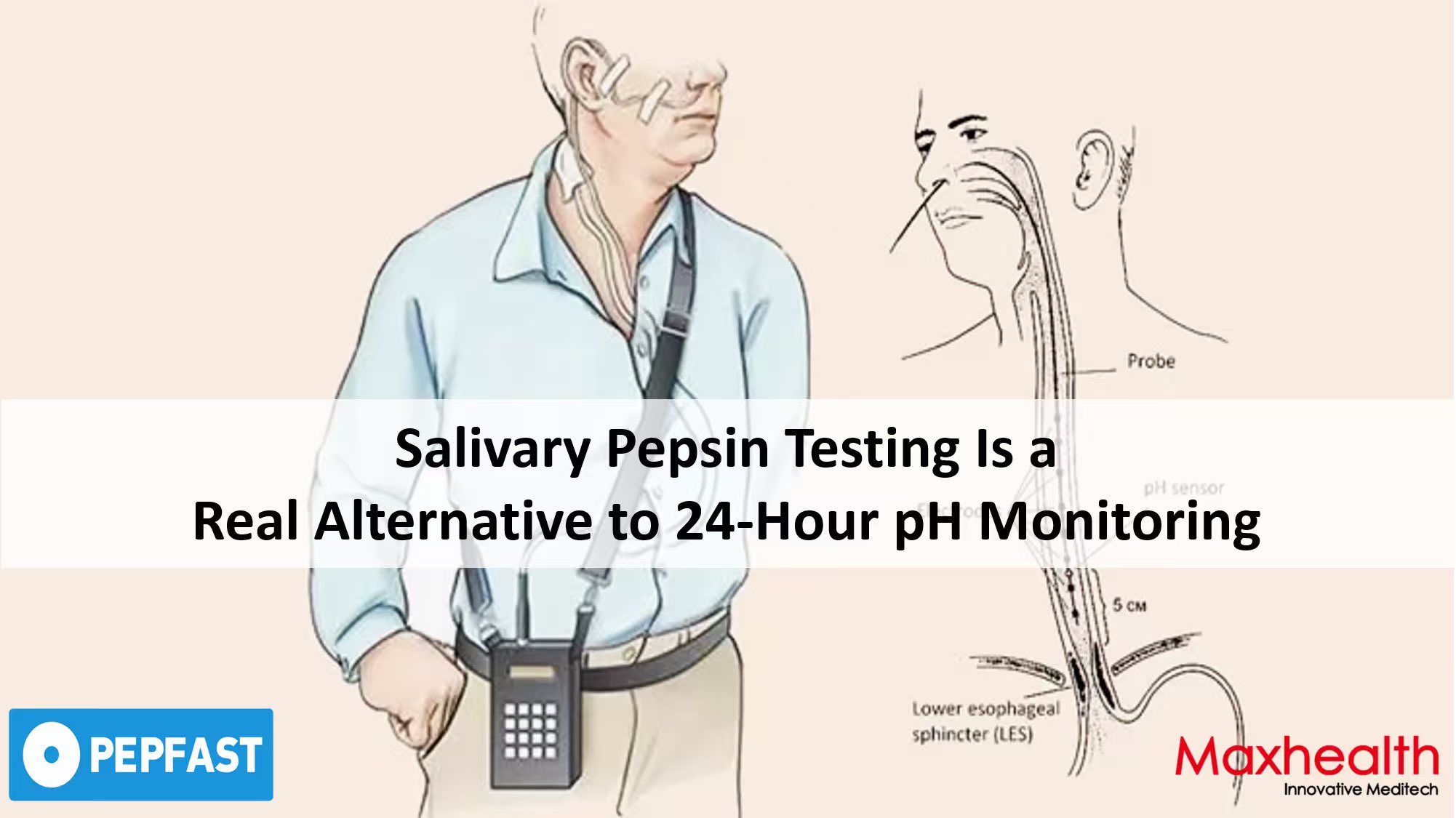
The 24‑hour ambulatory pH or impedance‑pH test typically requires transnasal placement of a thin catheter that remains in place for a full day. The procedure disrupts normal eating, sleeping and daily activities, and many patients find it poorly tolerated. Wireless capsule systems (e.g. Bravo) avoid the nasal tube but still need endoscopic placement and may not be widely available. At the same time, the diagnostic yield of 24‑hour monitoring is not as high as often assumed.
In patients with chronic laryngeal symptoms who underwent both wireless 48‑hour pH monitoring and 24‑hour impedance‑pH monitoring, the diagnostic yield was substantially lower with the 24‑hour catheter‑based test (27%) than with prolonged wireless monitoring (50%), despite both devices measuring the first 24 hours of the same study period [1]. This observation suggests that a single day of catheter‑based monitoring may miss clinically significant reflux that is captured over a longer period or with a less intrusive device. The implication is clear: a test that is quick, simple and repeatable could overcome many of these shortcomings.
How Salivary Pepsin Testing Works
Pepsin is a digestive enzyme produced exclusively in the gastric mucosa. Under physiological conditions, it should never appear in saliva, throat secretions or the airways. However, when gastric contents reflux upwards—whether acid, weakly acid or non‑acid—pepsin travels with them. Therefore, detecting pepsin in a saliva sample provides direct, objective proof that a reflux event has occurred up to the upper aerodigestive tract.
Salivary pepsin detection using a lateral flow device, such as Pepfast, is straightforward:
This simplicity allows the test to be performed in primary care clinics, ENT offices or even—under professional guidance—in homecare settings. The result is immediately available and can be discussed at the same consultation, dramatically reducing the time to diagnosis.
Comparative Clinical Evidence: Changing the Diagnostic Outcome
Several studies have directly compared salivary pepsin measurement with 24‑hour pH monitoring. One of the most striking findings comes from a 2015 UK study that enrolled 100 patients referred for catheter‑based 24‑hour pH monitoring. Participants collected up to three saliva samples at the time of their predominant reflux symptoms and underwent simultaneous manometry and pH monitoring. While pH monitoring classified only 49% of patients as having reflux disease, salivary pepsin measurement found that 81% of the same cohort had at least one positive pepsin sample. Furthermore, salivary pepsin changed the diagnostic outcome in 44% of symptomatic reflux patients when compared with pH monitoring alone [1].
The authors concluded that the higher proportion of pepsin‑positive patients “may reflect the poor sensitivity of 24‑hour pH monitoring” and that salivary pepsin measurement could help prevent false‑negative diagnoses based solely on pH data. In other words, a negative 24‑hour pH study does not reliably rule out reflux; a positive pepsin test can identify patients who would otherwise be told they do not have reflux and sent away without treatment.
Another systematic evaluation of the diagnostic utility of salivary pepsin compared with 24‑hour dual pH/impedance probe in LPR specifically concluded that salivary pepsin detection is a “simpler, more cost‑effective, and less traumatic universal first‑line alternative” to 24‑hour impedance‑pH probe in diagnosing LPR [2].
Which Test for Which Patient?
Both 24‑hour pH monitoring and salivary pepsin testing have a role in modern diagnostics, but they serve different purposes:
|
|
24‑Hour pH / Impedance Monitoring |
Salivary Pepsin Testing (Pepfast) |
|
Invasiveness |
High (catheter or endoscopic capsule placement) |
Non‑invasive (saliva sample only) |
|
Time to result |
24–48 hours after completion |
15 minutes from sample collection |
|
Equipment |
Specialized laboratory & software |
None; lateral flow device |
|
Reflux detected |
Acid exposure time; weakly acidic & non‑acid with impedance |
Any reflux event (acid or non‑acid) that contains pepsin |
|
Best for |
Quantifying acid burden; pre‑surgical evaluation; complex refractory cases |
First‑line screening, monitoring, LPR and extra‑esophageal symptoms |
|
Cost |
High (device, technician time, interpretation) |
Low |
The real value of salivary pepsin testing is not in replacing all pH monitoring, but in serving as an accessible, painless and rapidly repeatable triage tool. A patient with classic heartburn or chronic throat symptoms can be tested in the clinic at the first visit; if pepsin is detected, a diagnosis of reflux is strongly supported and treatment can begin immediately. If the result is negative but clinical suspicion remains high, the test can be repeated on different days or at different times (e.g. post‑prandial, after symptoms). Only if further quantification of acid burden is needed for surgical planning or for investigating refractory symptoms should the patient proceed to more extensive monitoring.
A non‑invasive alternative to 24‑hour pH monitoring addresses the most common patient complaints about traditional reflux testing: discomfort, disruption of daily life and delay in receiving a diagnosis. For clinicians, it offers an objective biomarker that is directly tied to the pathophysiology of reflux and does not rely on indirect measures such as pH alone. Moreover, because the test can be performed immediately in the office, the dreaded “try this medication for eight weeks and come back” approach can be replaced with evidence‑based decision‑making at the point of care.
A positive pepsin test provides a clear explanation for otherwise vague throat or chest symptoms; a negative test, especially when repeated on several occasions, helps redirect the diagnostic search toward other causes—without subjecting the patient to an unnecessary invasive procedure.
❓Frequently Asked Questions
1. Can salivary pepsin testing completely replace 24‑hour pH monitoring?
No. pH‑impedance monitoring remains important for quantifying acid burden, evaluating the adequacy of acid suppression therapy and selecting patients for anti‑reflux surgery. However, for first‑line screening, assessing LPR and monitoring treatment response, salivary pepsin testing is a practical, well‑validated alternative [1][2].
2. Is the test accurate enough to be trusted in clinical practice?
Yes. Large studies have demonstrated good sensitivity for detecting GERD and LPR. One study found that salivary pepsin changed the diagnostic outcome in 44% of symptomatic reflux patients compared with pH monitoring alone [1]. Another systematic review concluded that it is a reliable first‑line alternative to impedance‑pH testing [2].
3. Which patients are best suited for salivary pepsin testing?
The test is particularly valuable for patients with extra‑esophageal symptoms (chronic cough, hoarseness, globus sensation, throat clearing) who often have normal pH studies. It is also ideal for initial screening in primary care, for monitoring response to alginate therapy or lifestyle changes, and for patients who cannot tolerate or refuse invasive monitoring.
4. How should a clinician interpret a negative salivary pepsin test?
A single negative result does not completely exclude reflux, as reflux events are intermittent. If clinical suspicion remains high, the test should be repeated on different days at times when symptoms are most likely (e.g. post‑prandial, upon waking). A persistently negative salivary pepsin after three‑to‑four carefully timed samples makes reflux an unlikely cause and justifies investigation of alternative diagnoses.
References
[1] Rasijeff AMP, Jackson W, Burke JM, Dettmar PW. PWE‑172 Does salivary pepsin measurement change diagnostic outcome in patients investigated by 24h pH monitoring? Gut. 2015;64(Suppl 1): A287.3.
[2] Zhang M, Chia C, Stanley C, Phyland D, Paddle P. Diagnostic Utility of Salivary Pepsin as Compared With 24‑Hour Dual pH/Impedance Probe in Laryngopharyngeal Reflux. Otolaryngol Head Neck Surg. 2020;164(2):375‑380.
Medical Review by: Prof. Peter Dettmar, world‑renowned expert in reflux disease and the original developer of pepsin detection technology.









Copyright @ 2026 Maxhealth Innovative Meditech (Wuxi) Ltd All Rights Reserved.  Network Supported
Network Supported
Leave A Message
